
Ventricles
Ischemic
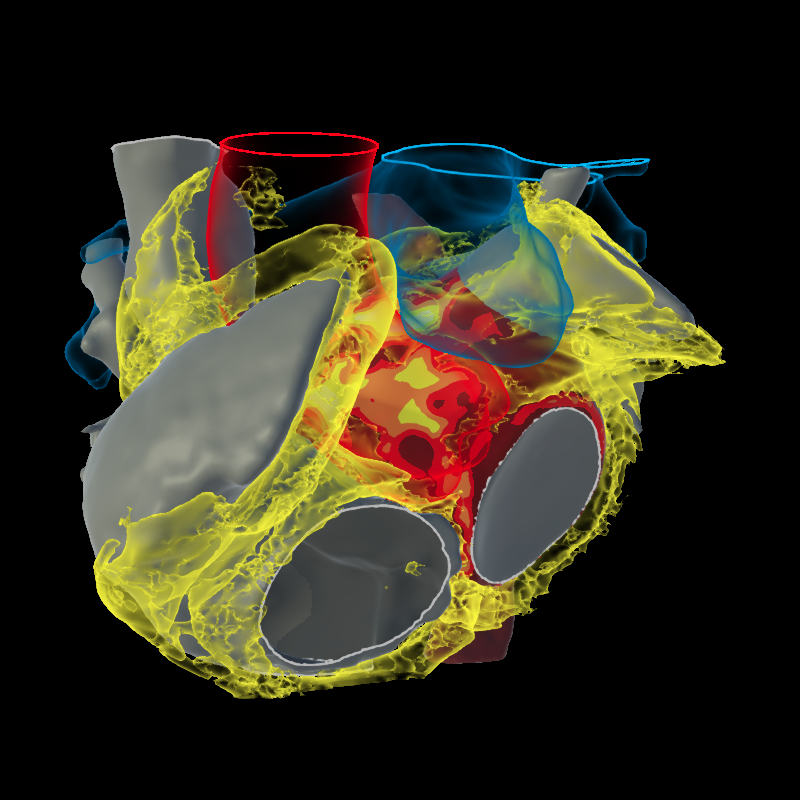
The most common VT etiology, our proprietary wall thinning rendering provides a roadmap for localizing spatial aspects of the scar and the critical isthmuses within the substrate that enable reentrant circuits. It allows more precise targeting and potentially less challenging mid-isthmus ablation targets compared to entrance/exit sites. These sites co-localize nicely with LAVA, ILAM and functional mapping/pacing maneuvers.

Ischemic
CT + Late CT
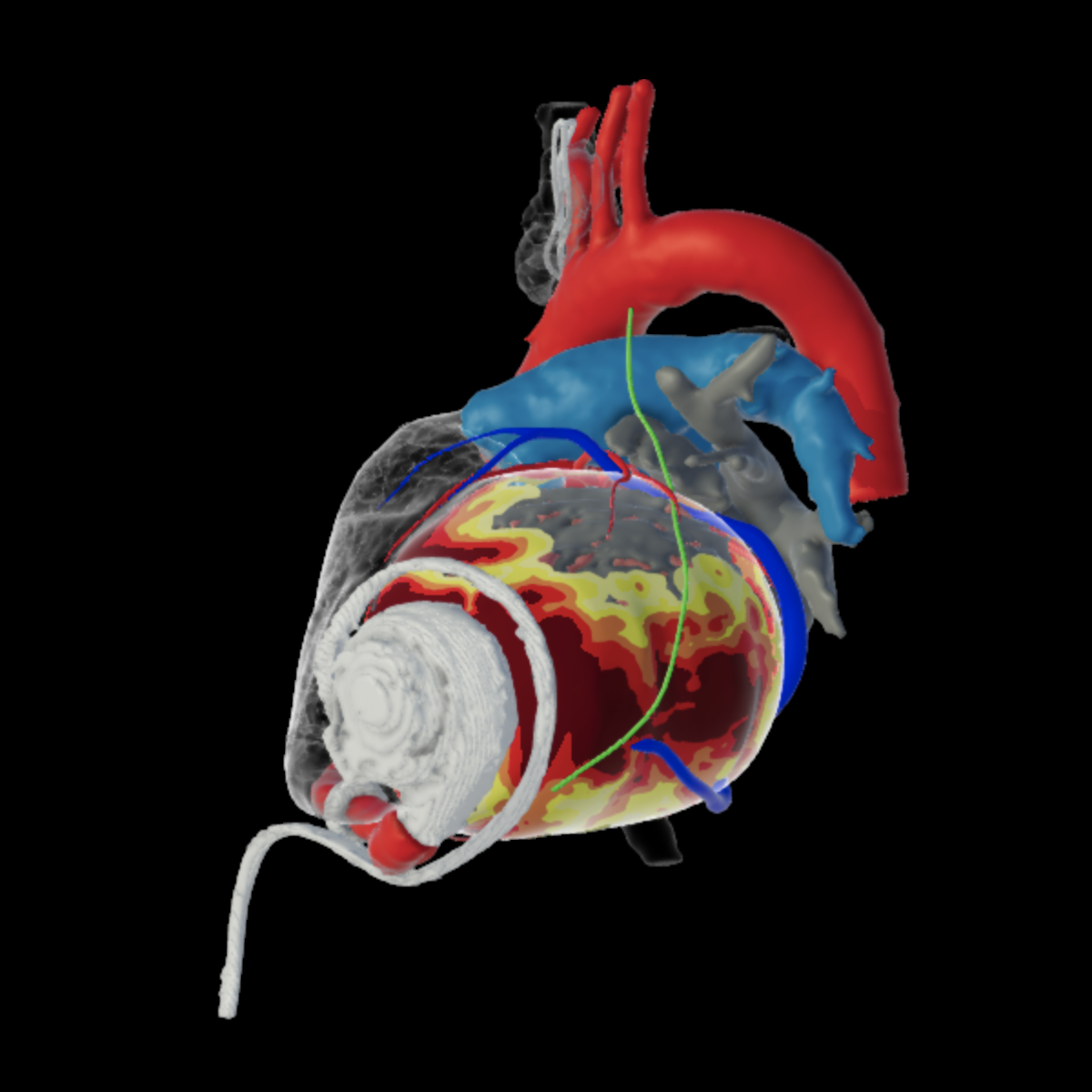
LVAD
CT
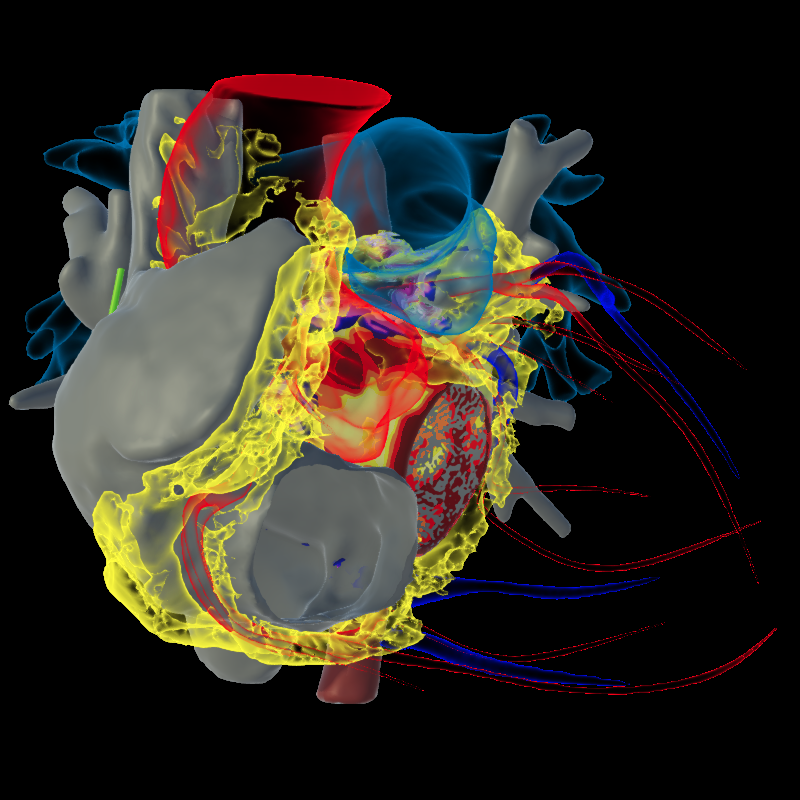
Non Ischemic
inHEART modeling characterizes the ventricular substrate in these difficult NICM scenarios. Scar transmurality, i.e., endocardial, mid-myocardial and epicardial scar is delineated, informing the mapping and ablation strategies prior to the procedure. Fatty infiltrate, calcifications and adipose fat are clearly rendered in these patients. Dark Core matter from previous ablation procedures help tell the tale of why the patient is again presenting with VT and may help guide additional therapy.

ARVC
CT

Cardiac Tumor
CT + MR

Dilated CMP
CT + Late CT

MR Transmurality
MR

Post myocarditis
CT + MR

Sarcoidosis
MR + PET CT
Congenital
Information about the extent of prior surgical interventions is not always available in this adult population. Visualizing complex anatomy, baffles, and surgical incisions that frequently sustain arrhythmias may reduce procedure time when the intervention is performed at a site different from the original surgery.

Fontan surgery
CT

Tetralogy of fallot
CT

Tetralogy of fallot
MR

Transposition of great vessels
CT
Atria
In patients with durable PVI and PWI who present with AF, assessing the atrial substrate for potential linear ablation or inducible triggers may be a useful strategy. Wall thickness data may inform the placement of transmural ablation lines in AF and left atrial flutters. Epicardial adipose tissue (EAT) infiltrate may be causative in this subset of patients.
Atrial Fibrillation
CT

Atrial Fibrillation
MR
Cardioneural Ablation
CT